Department of Orthopaedic Surgery, Wake Forest Baptist Health, Winston Salem, NC
Appointments: (336) 716-2011
Education
M.D. with Honors: Annual Medical Knowledge Olympics, 1st Place, among 7 medical
schools.
PhD in 3D joint kinematics, thesis published work has received 420 citations.
Residency at Wake Forest University Baptist Medical Center.
Fellowship at University of Washington, Seattle, WA (Drs Matsen, Warme)
Research
Basic Science in Biomechanics, Clinical Research Fellowship at Wake Forest University
Baptist Medical
Center. Overall have received 2000 citations for journal published work, 940 citations
since 2014.
Clinical care
Have performed a wide spectrum of orthopaedic surgery, from trauma to total joint
replacement surgery
and pediatric trauma. Since 2016 a more focused practice in Shoulder, Elbow and Hand
surgery.
Academic positions
Prior: University of Washington, Weill Cornell Medical College.
Current: Wake Forest School of Medicine, Winston Salem, NC -Uniformed Service: Infantry
Military,
Greek Public Health Service Military, Greek Public Health Service.
Experience
Assistant Professor
Wake Forest Baptist Health · Winston-Salem, NC December
2016 -
Present
Orthopaedic Surgery Wake Forest University
Health Sciences · Winston
Salem, NC October 2016 - Present
Affiliations
Wake Forest Baptist Health
Current
AffiliationWinston-Salem, NC
Wake Forest Baptist Medical Center
Current
AffiliationWinston-Salem, NC
NewYork-Presbyterian/Lower Manhattan Hospital
Former AffiliationNew York,
NY
New York Presbyterian Hospital Weill Cornell Medical College
Former AffiliationNew York, NY
University of Washington Medical Center
Former AffiliationSeattle, WA
Education & Training
University of Washington
Fellowship, Shoulder and Elbow, 2010
-
2011
Wake Forest University
Residency, Orthopedic
Surgery, 2006 -
2010
Wake Forest University
Internship, General
Surgery, 2005 -
2006
Bowman Gray School of Medicine Afl Hs
Post-Doctoral Fellowship, Orthopaedic
Surgery
Research, 2004 - 2005
University of Ioannina
PhD, Motion Analysis, 2000
-
2005
University of Ioannina
Class of 1999
Skills & Expertise
Osteoarthritis, Rotator cuff injuries, Shoulder surgery, Shoulder
and elbow
surgery, Total joint replacement, Hand and wrist functional reconstruction,
Orthopaedic traumatology,
Pediatric shoulder and elbow surgery,
Minimally invasive orthopaedic surgery, Orthopaedic implants, Joint preservation
surgery, Elbow medial
ulnar collateral ligament repair, Revision shoulder surgery, Complex shoulder
surgery, Motion analysis
and joint
kinematics, Clinical and outcomes research.
Certification & Licensure
NJ State Medical License
2015 - 2017
NY State Medical License
2015 - 2017
CA State Medical License
2014 - 2018
WA State Medical License
2010 - 2016
NC State Medical License
2010 - 2020
American Board of Orthopaedic Surgery
Orthopaedic Surgery
Awards, Honors & Recognition
Bear Award of Excellence
Southeastern
Health, 2013
Chair’s Award for Best Research
University of Washington, Department of
Orthopaedic
Surgery and Sports Medicine, 2011
Best poster award
Hellenic Association of Orthopaedics,
Surgery and
Traumatology, Athens, Greece, 2008
Silver Award
15th Annual Residents’ and Fellows’
Research Day,
Division of Surgical Sciences. Wake Forest University, 2006
Gold Medal
12th Annual Residents’ and Fellows’
Research Day,
Division of Surgical Sciences. Wake Forest University School of Medicine, Winston Salem,
NC,
USA, 2004
Contact info: Department of
Orthopaedic Surgery, Wake Forest University Baptist Health, 131 Miller St, Winston Salem, NC 27103
Appointments:
336-7168200
RESEARCH
Basic Science in Biomechanics,
Clinical Research Fellowship at Wake Forest University Baptist Medical Center, Clinical Shoulder
and Elbow Fellowship at University of Washington, Seattle, WA
Jinnah AH, Luo TD, Wiesler ER, Li Z, Poehling GG, Tuohy CJ, Graves BR,
Freehill MT, Papadonikolakis A. Peripheral Nerve Injury After Elbow Arthroscopy:
An Analysis of Risk Factors. Arthroscopy. 2018 May;34(5):1447-1452. doi:
10.1016/j.arthro.2017.12.004. PubMed PMID: 29398211.
Papadonikolakis A. Arthroscopic Reduction and Fixation of Transverse
Intra-articular Glenoid Fractures With Scapular Extension. Arthrosc Tech. 2017
Jun 26;6(3):e879-e885. doi: 10.1016/j.eats.2017.02.018. eCollection 2017 Jun.
PubMed PMID: 28706846; PubMed Central PMCID: PMC5495986.
Nunez FA, Papadonikolakis A, Li Z. Arthroscopic Release of Adhesive
Capsulitis
of the Shoulder Complicated With Shoulder Dislocation and Brachial Plexus Injury.
J Surg Orthop Adv. 2016 summer;25(2):114-6. PubMed PMID: 27518297.
Papadonikolakis A, Matsen FA 3rd. Metal-Backed Glenoid Components Have a
Higher Rate of Failure and Fail by Different Modes in Comparison with
All-Polyethylene Components: A Systematic Review. J Bone Joint Surg Am. 2014 Jun
18;96(12):1041-1047. Review. PubMed PMID: 24951741.
Papadonikolakis A, Neradilek MB, Matsen FA 3rd. Failure of the glenoid
component in anatomic total shoulder arthroplasty: a systematic review of the
English-language literature between 2006 and 2012. J Bone Joint Surg Am. 2013 Dec
18;95(24):2205-12. doi: 10.2106/JBJS.L.00552. Review. PubMed PMID: 24352774.
Matsen FA 3rd, Papadonikolakis A. Published evidence demonstrating the
causation of glenohumeral chondrolysis by postoperative infusion of local
anesthetic via a pain pump. J Bone Joint Surg Am. 2013 Jun 19;95(12):1126-34.
doi: 10.2106/JBJS.L.01104. Review. PubMed PMID: 23783210.
Papadonikolakis M, Bouganis CS. Novel cascade FPGA accelerator for support
vector machines classification. IEEE Trans Neural Netw Learn Syst. 2012
Jul;23(7):1040-52. doi: 10.1109/TNNLS.2012.2196446. PubMed PMID: 24807131.
Papadonikolakis A, McKenna M, Warme WJ, Matsen FA. Intramedullary fibular and
impaction allografting in revision total elbow arthroplasty with endosteal
deficiency. Tech Hand Up Extrem Surg. 2012 Mar;16(1):5-11. doi:
10.1097/BTH.0b013e318225475d. PubMed PMID: 22370364.
Papadonikolakis A, McKenna M, Warme W, Martin BI, Matsen FA 3rd.
Published
evidence relevant to the diagnosis of impingement syndrome of the shoulder. J
Bone Joint Surg Am. 2011 Oct 5;93(19):1827-32. doi: 10.2106/JBJS.J.01748. Review.
PubMed PMID: 22005869.
Wiesler ER, Sarlikiotis T, Rogers S, Papadonikolakis A, Poehling GG.
Arthroscopic debridement for osteochondral injury of the elbow trochlea: a case
report with a long-term follow-up. J Shoulder Elbow Surg. 2011 Mar;20(2):e18-22.
doi: 10.1016/j.jse.2010.09.015. Epub 2010 Dec 30. PubMed PMID: 21194978.
Ruch DS, Wray WH 3rd, Papadonikolakis A, Richard MJ, Leversedge FJ, Goldner
RD. Corrective osteotomy for isolated malunion of the palmar lunate facet in
distal radius fractures. J Hand Surg Am. 2010 Nov;35(11):1779-86. doi:
10.1016/j.jhsa.2010.07.036. Epub 2010 Oct 20. PubMed PMID: 20961709.
Lucado AM, Li Z, Russell GB, Papadonikolakis A, Ruch DS. Changes in
impairment and function after static progressive splinting for stiffness after
distal radius fracture. J Hand Ther. 2008 Oct-Dec;21(4):319-25. doi:
10.1197/j.jht.2008.01.002. PubMed PMID: 19006757.
Chloros GD, Papadonikolakis A, Ginn S, Wiesler ER. Pronator quadratus space
and compartment syndrome after low-energy fracture of the distal radius: a case
report. J Surg Orthop Adv. 2008 Summer;17(2):102-6. PubMed PMID: 18549742.
Ruch DS, Shen J, Chloros GD, Krings E, Papadonikolakis A. Release of the
medial collateral ligament to improve flexion in post-traumatic elbow stiffness.
J Bone Joint Surg Br. 2008 May;90(5):614-8. doi: 10.1302/0301-620X.90B5.19999.
PubMed PMID: 18450628.
Papadonikolakis A, Wiesler ER, Olympio MA, Poehling GG. Avoiding
catastrophic
complications of stroke and death related to shoulder surgery in the sitting
position. Arthroscopy. 2008 Apr;24(4):481-2. doi: 10.1016/j.arthro.2008.02.005.
Review. PubMed PMID: 18375282.
Chloros GD, Wiesler ER, Stabile KJ, Papadonikolakis A, Ruch DS, Kuzma GR.
Reconstruction of essex-lopresti injury of the forearm: technical note. J Hand
Surg Am. 2008 Jan;33(1):124-30. doi: 10.1016/j.jhsa.2007.09.008. Review. PubMed
PMID: 18261676.
Papadonikolakis A, Chloros GD, Smith BP, Koman LA. Digital ischemia due to
essential thrombocythemia: a case report. J Hand Surg Am. 2007 Sep;32(7):1053-7.
PubMed PMID: 17826562.
Chloros GD, Papadonikolakis A, Themistocleous GS. Correlation of
high-resolution ultrasonographic findings with the clinical symptoms and
electrodiagnostic data in carpal tunnel syndrome. Ann Plast Surg. 2007
Sep;59(3):351-2. PubMed PMID: 17721230.
Ruch DS, Papadonikolakis A, Campolattaro RM. The posterolateral plica: a
cause of refractory lateral elbow pain. J Shoulder Elbow Surg. 2006
May-Jun;15(3):367-70. PubMed PMID: 16679240.
Ruch DS, Papadonikolakis A. Resection of the scaphoid distal pole for
symptomatic scaphoid nonunion after failed previous surgical treatment. J Hand
Surg Am. 2006 Apr;31(4):588-93. PubMed PMID: 16632052.
Papadonikolakis A, Li Z, Smith BP, Koman LA. Fractures of the phalanges
and
interphalangeal joints in children. Hand Clin. 2006 Feb;22(1):11-8. Review.
PubMed PMID: 16504774.
Ruch DS, Papadonikolakis A. Volar versus dorsal plating in the management
of
intra-articular distal radius fractures. J Hand Surg Am. 2006 Jan;31(1):9-16.
PubMed PMID: 16443097.
Shen J, Papadonikolakis A, Garrett JP, Davis SM, Ruch DS. Ulnar-positive
variance as a predictor of distal radioulnar joint ligament disruption. J Hand
Surg Am. 2005 Nov;30(6):1172-7. PubMed PMID: 16344174.
Ruch DS, Lumsden BC, Papadonikolakis A. Distal radius fractures: a
comparison
of tension band wiring versus ulnar outrigger external fixation for the
management of distal radioulnar instability. J Hand Surg Am. 2005
Sep;30(5):969-77. PubMed PMID: 16182053.
Ruch DS, Papadonikolakis A. Arthroscopically assisted repair of
peripheral
triangular fibrocartilage complex tears: factors affecting outcome. Arthroscopy.
2005 Sep;21(9):1126-30. PubMed PMID: 16171639.
Papadonikolakis A, Ruch DS. Internal distraction plating of distal radius
fractures. Tech Hand Up Extrem Surg. 2005 Mar;9(1):2-6. Review. PubMed PMID:
16092812.
Papadonikolakis A, Shen J, Garrett JP, Davis SM, Ruch DS. The effect of
increasing distraction on digital motion after external fixation of the wrist. J
Hand Surg Am. 2005 Jul;30(4):773-9. PubMed PMID: 16039371.
Georgoulis AD, Ristanis S, Papadonikolakis A, Tsepis E, Moebius U, Moraiti
C,
Stergiou N. Electromechanical delay of the knee extensor muscles is not altered
after harvesting the patellar tendon as a graft for ACL reconstruction:
implications for sports performance. Knee Surg Sports Traumatol Arthrosc. 2005
Sep;13(6):437-43. Epub 2005 Jun 21. PubMed PMID: 15968530.
Mavrodontidis AN, Zalavras CG, Papadonikolakis A, Soucacos PN. Bilateral
absence of the patella in nail-patella syndrome: delayed presentation with
anterior knee instability. Arthroscopy. 2004 Oct;20(8):e89-93. PubMed PMID:
15483536.
Papadonikolakis AS, Vekris MD, Korompilias AV, Kostas JP, Ristanis SE,
Soucacos PN. Botulinum A toxin for treatment of lower limb spasticity in cerebral
palsy: gait analysis in 49 patients. Acta Orthop Scand. 2003 Dec;74(6):749-55.
PubMed PMID: 14763710.
Papadonikolakis A, Mavrodontidis AN, Zalavras C, Hantes M, Soucacos PN.
Transscaphoid volar lunate dislocation. A case report. J Bone Joint Surg Am. 2003
Sep;85(9):1805-8. PubMed PMID: 12954842.
Papadonikolakis AS, Vekris MD, Kostas JP, Korompilias AV, Soucacos PN.
Transient erectile dysfunction associated with intramuscular injection of
botulinum toxin type A. J South Orthop Assoc. 2002 Summer;11(2):116-8. PubMed
PMID: 12741592.
Mavrodontidis AN, Papadonikolakis A, Moebius UG, Gelalis I, Motsis E,
Soucacos PN. Posterior tibial subluxation and short-term arthritis resulting from
failed posterior cruciate ligament reconstruction. Arthroscopy. 2003
May-Jun;19(5):E43. PubMed PMID: 12724667.
Papadonikolakis A, Cooper L, Stergiou N, Georgoulis AD, Soucacos PN.
Compensatory mechanisms in anterior cruciate ligament deficiency. Knee Surg
Sports Traumatol Arthrosc. 2003 Jul;11(4):235-43. Epub 2003 Apr 17. Review.
PubMed PMID: 12700888.
Georgoulis AD, Papadonikolakis A, Papageorgiou CD, Mitsou A, Stergiou N.
Three-dimensional tibiofemoral kinematics of the anterior cruciate
ligament-deficient and reconstructed knee during walking. Am J Sports Med. 2003
Jan-Feb;31(1):75-9. PubMed PMID: 12531761.
Georgoulis AD, Papageorgiou CD, Moebius UG, Rossis J, Papadonikolakis A,
Soucacos PN. The diagnostic dilemma created by osteoid osteoma that presents as
knee pain. Arthroscopy. 2002 Jan;18(1):32-7. PubMed PMID: 11774139.
Moebius UG, Georgoulis AD, Papageorgiou CD, Papadonikolakis A, Rossis J,
Soucacos PN. Alterations of the extensor apparatus after anterior cruciate
ligament reconstruction using the medial third of the patellar tendon.
Arthroscopy. 2001 Nov-Dec;17(9):953-9. PubMed PMID: 11694927.
Clinical Work
Clinical work performed in my practice includes surgery of the shoulder elbow and hand.
Prior to joining Wake
Forest University Baptist medical center my focus was on trauma, joint replacement surgery in addition to
the field of upper extremity surgery. Since 2016 my practice is more focused on the upper extremity
surgery.
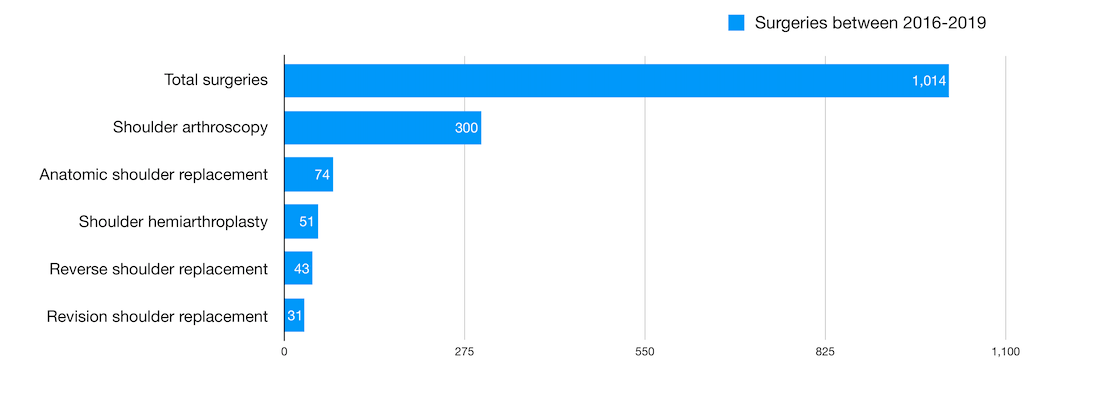
High volume shoulder replacement surgeon is considered a surgeon who performs 10 shoulder replacements
per year.
My experience in the upper extremity surgery has been extensive, especially after completion of the shoulder
and elbow fellowship at the University of Washington (UW), Seattle, WA in 2011. The UW program is one of the
busiest shoulder programs in the country. On average during the 12 months that I spend there, we performed
12 shoulder arthroplasties per week including one to two revisions per week. This was the
foundation of my advanced clinical experience in the field of shoulder and elbow surgery. During that year
(2011) we studied three major problems in the field of shoulder surgery, all three were published in the
JBJS journal (Journal of Bone and Joint Surgery, Am.)
Metal backed glenoid components (Our analysis included data on 1571 metal-backed and 3035
all-polyethylene components. The mean duration of follow-up was 5.8 years in the studies with
metal-backed components and 7.3 years with all-polyethylene components.)
Failure of the glenoid component in anatomic shoulder replacement. Data from 3853 total shoulder
arthroplasties performed from 1976 to 2007 were analyzed
Shoulder impingement syndrome: More than 2500 articles on the subject were reviewed and recommendations
were made on the use of the term "impingement".
OrthoMesh3D
Plan orthopaedic surgery in 3D using Blender
I am the developer of the OrthoMesh3D software and online course which is hosted by Udemy, Inc. The software
is a platform for the computer graphics integrated software Blender written in Python. The OrthoMesh3D is
utilized in planning and visualizing surgical plans in orthopaedic surgery. As of May 2020, the 9 hour
course had international attendance with over 70 participants from 19 countries within one month from its
release date (April 2020).
This course covers the basics of the free open source software named Blender, and how to utilize
it in the
planning of orthopaedic surgery using 3D bone models from CT scans. The modeling and animation of bones and
joints is covered, as well as the principles of deformity correction using cutting guides in the 3D
environment using the Add on script - OrthoMesh3D. Explanations are given on converting DICOM CT scans to 3D
bone models, and importing them into Blender for surgical planning. There is a detailed explanation on how
to use the free software Inkscape for converting pictures of implants to SVG files which then can be
converted into 3D models in Blender. Lastly, case examples of shoulder replacement surgery are provided in
addition to animation and simulation methods using the Blender's Armature tool. Inverse and Forward
Kinematics for joint and bone model animation is covered too. The processes described in this course and
software used are for research and virtual planning, NON FDA approved software is used. Not intended for
clinical use in the USA.
Who this course is for:
Surgeons, Medical Personnel, Engineers, Implant companies, Physicians, Medical Students
Python developers, Radiology physicians, Students or Instructors of Anatomy of the Musculoskeletal System
The hemiarthroplasty of the shoulder, is a partial replacement of the shoulder joint (ball and
socket mechanism). During this procedure the humeral head (ball) is replaced with a metallic ball in
an
attempt to restore (a) smoothness of the surface (b) sphericity of the humeral head.
The metallic implant has a stem that is press fitted into the
bone canal – humeral canal. The
prosthetic metallic head is attached to the stem of the implant with a morse taper
mechanism.
Arthritis of the humeral head – ball with loss of sphericity and smoothness of the ball
Indications:
A hemiarthroplasty is commonly used in the following clinical scenarios
Arthritis of the shoulder in a young patient, <60-65 years old, with high levels of activity
Proximal humeral fractures – fractured ball in many pieces that is not amendable to fixation
using screws and plates
Revision surgery of prior failed shoulder replacement
Avascular necrosis of the ball – humeral head, usually seen in younger patients
When there is insufficient bone left in the socket – glenoid of the shoulder – and a total
shoulder replacement cannot be done because the socket cannot support an implant.
Technique:
A simulation of the replaced shoulder with a hemiarthroplasty is demonstrated in the video
below. This was done using the software OrthoMesh3D that I developed and use for preoperative
planning.
Rehabilitation:
The rehabilitation after hemiarthroplasty requires immobilization of the shoulder in a sling for 6
weeks. This is necessary to allow the muscles of the shoulder to heal as those are separated and
then repaired after implantation of the prosthesis. It is crucial to avoid forceful internal or
external rotation of the shoulder- such as opening or closing doors with the arm. During those 6
weeks the sling can be removed for therapy and passive range of motion of the shoulder. After 6
weeks the sling is discontinued and light strengthening is started with progressive supine bench
pressing, as well as scapular muscle and deltoid muscle strengthening. Patients experience the full
benefit of surgery between 6-12 months from surgery.
Results:
The results of hemiarthroplasty in terms of relief of pain are inferior to those of a total shoulder
replacement – replacing the ball and socket of the shoulder. However, the benefit of the
hemiarthroplasty is that it does not require any limitation in activity. After 6 months patients are
allowed to do anything they wish to do. With the total shoulder replacement heavy activity is not
permitted as this level of activity will result in early failure of the implant. The relief in pain
from a hemiarthroplasty can be full, however most of the time is partial. The main reasons for a
revision of a hemiarthroplasty is stiffness, erosion of the socket – glenoid of the shoulder- from
the metallic ball, infection, or hardware complications such as loosening. Stiffness can be managed
sometimes with gentle manipulation under conscious sedation. The frequency of those complications is
somewhere between 4-10%.
Distal Radius Fractures
Introduction:
Distal radius fractures are the most common fractures of the arm. The radius is the larger of the two
bones of the forearm. The end toward the wrist is called the distal end. A fracture of the distal
radius occurs when the area of the radius near the wrist breaks. Distal radius fractures are very
common. In fact, the radius is the most commonly broken bone in the arm.
Intra-articular fracture. A fracture that extends into the wrist joint. ("Articular" means
"joint.")
Extra-articular fracture. A fracture that does not extend into the joint is called an
extra-articular fracture.
Open fracture. When a fractured bone breaks the skin, it is called an open fracture. These types
of fractures require immediate medical attention because of the risk for infection.
Comminuted fracture. When a bone is broken into more than two pieces, it is called a comminuted
fracture.
The most common cause of a distal radius fracture is a fall onto an outstretched arm.
Osteoporosis (a disorder in which bones become very fragile and more likely to break) can make a
relatively minor fall result in a broken wrist. Many distal radius fractures in people older than 60
years of age are caused by a fall from a standing position.
A broken wrist can happen even in healthy bones, if the force of the trauma is severe enough. For
example, a car accident or a fall off a bike may generate enough force to break a wrist.
Good bone health remains an important prevention option. Wrist guards may help to prevent some
fractures, but they will not prevent them all.
Treatment
The treatment of this fracture depends on the displaced, angulation of the fracture, deformity,
activity level of the patient, patient’s age and occupation, presence or absence of osteoporosis.
The treatment options are bracing, casting or surgery. Whether surgical treatment is required will
depend of patient’s preference and most importantly the doctor’s recommendation. During surgery
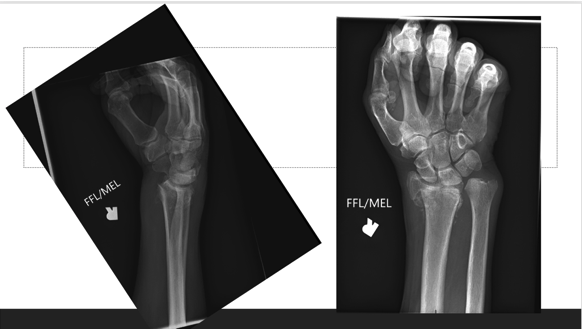
metallic implants – plates and screws – are used for fixation of the fracture. Below you will see
xrays prior and after surgery and fixation of the fracture with a plate and screws.
Picture on the left shows the fracture and on the right fixation with a plate.
Xrays below show a malunion – united bone in a displaced position – which required an osteotomy,
braking the bone again and fixing it.
The animation below shows the planning for the osteotomy using custom drilling and cutting
guides.
Recovery
Because the kinds of distal radius fractures are so varied and the treatment options are so broad,
recovery is different for each individual. Talk to your doctor for specific information about your
recovery program and return to daily activities.
Pain Management
Most fractures hurt moderately for a few days to a couple of weeks. Many patients find that using
ice, elevation (holding their arm up above their heart), and simple, non-prescription medications
for pain relief are all that are needed to relieve pain.
Your doctor may recommend combining ibuprofen and acetaminophen to relieve pain and inflammation.
The combination of both medications is much more effective than either one alone. If pain is severe,
your doctor may suggest a prescription-strength medication, such as an opioid, for a few days.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be
addictive. It is important to use opioids only as directed by your doctor. As soon as your pain
begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve
within a few days of your surgery.
Cast and Wound Care
In some cases, original casts will be replaced because swelling has gone down so much that the cast
becomes loose. The last cast is usually removed after about 6 weeks.
During healing, casts and splints must be kept dry. A plastic bag over the arm while showering
should help. If the cast does become wet, it will not dry very easily. A hair dryer on the cool
setting may be helpful.
Most surgical incisions must be kept clean and dry for 5 days or until the sutures (stitches) are
removed, whichever occurs later.
Potential Complications
After surgery or casting, it is important that you achieve full motion of your fingers as soon as
possible. If you are not able to fully move your fingers within 24 hours due to pain and/or
swelling, contact your doctor for evaluation.
Your doctor may loosen your cast or surgical dressing. In some cases, working with a physical or
occupational therapist will be required to regain full motion.
Unrelenting pain may be a sign of Complex Regional Pain Syndrome (Reflex Sympathetic Dystrophy)
which must be treated aggressively with medication or nerve blocks.
Rehabilitation and Return to Activity
Most people do return to all their former activities after a distal radius fracture. The nature of
the injury, the kind of treatment received, and the body's response to the treatment all have an
impact, so the answer is different for each individual.
Almost all patients will have some stiffness in the wrist. This will generally lessen in the month
or two after the cast is taken off or after surgery, and continue to improve for at least 2 years.
If your doctor thinks it is needed, you will start physical therapy within a few days to weeks after
surgery, or right after the last cast is taken off.
Most patients will be able to resume light activities, such as swimming or exercising the lower body
in the gym, within 1 to 2 months after the cast is removed or within 1 to 2 months after surgery.
Vigorous activities, such as skiing or football, may be resumed between 3 and 6 months after the
injury.
Long-Term Outcomes
Recovery should be expected to take at least a year.
Some pain with vigorous activities may be expected for the first year. Some residual stiffness or
ache is to be expected for 2 years or possibly permanently, especially for high-energy injuries
(such as motorcycle crashes), in patients older than 50 years of age, or in patients who have some
osteoarthritis. However, the stiffness is usually minor and may not affect the overall function of
the arm.
Finally, osteoporosis is a factor in many wrist fractures. It has been suggested that people who
have a wrist fracture should be tested for bone weakness, especially if they have other risk factors
for osteoporosis. Ask your doctor about osteoporosis testing.
Research
I have been the author or co-author of several studies on the subject of distal radius fractures and
I have classified 2500 xrays of the fractures of the distal radius for research purposes during my
study of those injuries. A sample of publications on the subject is shown below.
Ruch DS, Wray WH 3rd, Papadonikolakis A, Richard MJ, Leversedge FJ, Goldner RD. Corrective
osteotomy for isolated malunion of the palmar lunate facet in distal radius fractures. J Hand
Surg Am. 2010 Nov;35(11):1779-86. doi: 10.1016/j.jhsa.2010.07.036. Epub 2010 Oct 20. PubMed
PMID: 20961709.
Lucado AM, Li Z, Russell GB, Papadonikolakis A, Ruch DS. Changes in impairment and function
after static progressive splinting for stiffness after distal radius fracture. J Hand Ther. 2008
Oct-Dec;21(4):319-25. doi: 10.1197/j.jht.2008.01.002. PubMed PMID: 19006757.
Chloros GD, Papadonikolakis A, Ginn S, Wiesler ER. Pronator quadratus space and compartment
syndrome after low-energy fracture of the distal radius: a case report. J Surg Orthop Adv. 2008
Summer;17(2):102-6. PubMed PMID: 18549742.
Ruch DS, Papadonikolakis A. Volar versus dorsal plating in the management of intra-articular
distal radius fractures. J Hand Surg Am. 2006 Jan;31(1):9-16. PubMed PMID: 16443097.
Shen J, Papadonikolakis A, Garrett JP, Davis SM, Ruch DS. Ulnar-positive variance as a predictor
of distal radioulnar joint ligament disruption. J Hand Surg Am. 2005 Nov;30(6):1172-7. PubMed
PMID: 16344174.
Ruch DS, Lumsden BC, Papadonikolakis A. Distal radius fractures: a comparison of tension band
wiring versus ulnar outrigger external fixation for the management of distal radioulnar
instability. J Hand Surg Am. 2005 Sep;30(5):969-77. PubMed PMID: 16182053.
Papadonikolakis A, Ruch DS. Internal distraction plating of distal radius fractures. Tech Hand
Up Extrem Surg. 2005 Mar;9(1):2-6. Review. PubMed PMID: 16092812.
Papadonikolakis A, Shen J, Garrett JP, Davis SM, Ruch DS. The effect of increasing distraction
on digital motion after external fixation of the wrist. J Hand Surg Am. 2005 Jul;30(4):773-9.
PubMed PMID: 16039371.
Elbow Fracture
Introduction:
Trauma to the elbow is quite common. It may be a result of an isolated injury or combined with other
injuries of the arm. Taking into account age and the mechanism of injury is crucial, particularly
because of the risk of accompanying nerve or vascular injury.
For an understanding of the elbow anatomy and fractures please see the animation below:
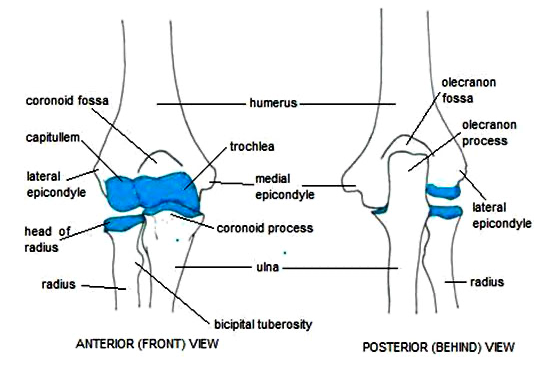
Summary of anatomy:
The elbow consists of portions of all three bones:
The distal humerus is the lower end of humerus. It forms the upper part of the elbow and is the
spool around which the forearm bends and straightens.
The radial head is the knobby end of the radius where it meets the elbow. It glides up and down the
front of the distal humerus when you bend your arm and rotates around the ulna when you turn your
wrist up or down.
The olecranon is the part of the ulna that "cups" the lower end of the humerus, creating a hinge for
elbow movement. The bony "point" of the olecranon can be easily felt beneath the skin because it is
covered by just a thin layer of tissue.
The elbow is held together by its bony architecture, as well as ligaments, tendons, and muscles.
Three major nerves cross the elbow joint.
Mechanism of injury
There are a variety of possible injuries because of the presence of three bones and the range of
mechanisms of injury.
Mechanism of injury in elbow fractures and dislocation
Radial head and neck fractures
Fall on to an outstretched hand
Olecranon fractures
Elderly - indirect trauma by pull of triceps and brachioradialis
Children - direct blow to elbow
Fractures of the coronoid process
Fall on to an extended elbow as for elbow dislocation
Fractures of the distal humerus
Fall on to an extended outstretched hand
Intercondylar fractures
Direct or indirect blow to elbow
Condylar fractures
Direct blow to a flexed elbow
Capitellum fracture
Fall on to an outstretched hand, or direct trauma
Elbow dislocation
Fall on to an extended elbow
Common in sport in the young
Radial head and neck fractures
Mechanism of injury
These are most commonly caused by a fall on to an outstretched arm. Radial head fracture is the most
common fracture around the elbow joint in adults, whereas radial neck fractures occur more commonly
in children.
Clinical features
The patient presents with swelling over the lateral elbow with limited range of motion,
particularly forearm rotation and elbow extension ± elbow effusion and bruising. Pain is
increased with passive rotation.
The most reliable clinical sign is point tenderness over the radial head.
Needs careful assessment for nerve and vascular involvement, especially with brachial artery,
median and ulnar nerves.
It is important to detect crepitation or a mechanical blockage of motion from displaced fracture
fragments. This often requires aspiration of a haemarthrosis – blood within elbow joint - with
the instillation of local anaesthetic for pain relief.
If there is significant wrist pain and/or central forearm pain, there may be acute longitudinal
radioulnar dissociation with disruption of the distal radioulnar joint.
Investigations
AP and lateral X-ray views of the elbow are usually sufficient.
Treatment
Doctors classify fractures according to the degree of displacement (how far out of normal position
the bones are). Treatment is determined by the type of fracture, according to the classification
below.
Type I Fractures
Type I fractures are generally small, like cracks, and the bone pieces remain fitted together.
The fracture may not be visible on initial x-rays, but can usually be seen if the x-ray is taken
3 weeks after the injury.
Nonsurgical treatment involves using a splint or sling for a few days, followed by an early and
gradual increase in elbow and wrist movement (depending on the level of pain).
If too much motion is attempted too quickly, the bones may shift and become displaced.
Type II Fractures
Type II fractures are slightly displaced and involve a larger piece of bone.
If displacement is minimal, a sling or splint may be used for 1 to 2 weeks, followed by
range-of-motion exercises.
Small fragments of broken bone may be surgically removed if they prevent normal elbow movement
or could cause long-term problems with the elbow.
If a fragment is large and out of place enough, the orthopaedic surgeon will first attempt to
hold the bones together with screws, or a plate and screws. If this is not possible, the surgeon
will remove the broken pieces of the radial head.
The surgeon will also correct any other soft-tissue injury, such as a torn ligament.
Type III Fractures
Type III fractures have multiple broken pieces of bone which cannot be put back together for healing.
In most Type III radial head fractures, there is also significant damage to the elbow joint and
the ligaments that surround the elbow.
Surgery is always required to either fix or remove the broken pieces of bone and repair the
soft-tissue damage. If the damage is severe, the entire radial head may need to be removed. In
some cases, an artificial radial head may be placed to improve long-term function.
Early movement to stretch and bend the elbow is necessary to avoid stiffness.
Even the simplest of fractures may result in some loss of movement in the elbow. Regardless of the
type of fracture or the treatment used, exercises to restore movement and strength will be needed
before resuming full activities.
Olecranon fractures
Mechanism of injury
These are low-energy fractures which occur most commonly in the elderly and result from indirect
trauma caused by a sudden pull of the triceps and brachioradialis muscles.
However, in younger patients, olecranon fractures usually follow a direct blow to the point of the
elbow and are often comminuted, and there may be an associated ulnar shaft fracture.
Clinical features
The patient presents with swelling and tenderness over the olecranon with haemarthrosis and
limited range of motion.
There is an inability to extend the elbow against gravity, indicating dysfunction of the triceps
lever.
There is a need to check for ulnar nerve damage and examine distal pulses.
Investigations
True lateral X-ray of the elbow should reveal the fracture.
Management
While you are in the emergency room, your doctor will apply a splint (like a cast) to your elbow, and
give you a sling to help keep the elbow in position. Immediate treatment may also include:
Applying ice to reduce pain and swelling
Medications to relieve pain
Whether or not your fracture requires surgery will be determined. Not all olecranon fractures
will require surgery.
Nonsurgical Treatment
If the pieces of bone are not out of place (displaced), a fracture can sometimes be treated with
a splint to hold the elbow in place during healing. During the healing process, your doctor will
take frequent x-rays to make sure the bone has not shifted out of place.
Splints are typically worn for 6 weeks before gentle motion is started. If the fracture shifts
in position during this time, you may need surgery to put the bones back together.
Surgical treatment
Surgery is usually required for olecranon fractures in which:
The bones have moved out of place (displaced fracture)
Pieces of bone have punctured the skin (open fracture)
Surgery for olecranon fractures typically involves putting the broken pieces of bone back into
position and preventing them from moving out of place until they are healed.
Because of the increased risk of infection, open fractures are scheduled for surgery as soon as
possible, usually within hours. Patients are given antibiotics by vein (intravenous) in the
emergency room, and may receive a tetanus shot. During surgery, the cuts from the injury and the
surfaces of the broken bone are thoroughly cleaned out. The bone will typically be repaired during
the same surgery.
Surgical Procedures
Open reduction and internal fixation. This is the procedure most often used to treat olecranon
fractures. During the procedure, the bone fragments are first repositioned (reduced) into their
normal alignment. The pieces of bone are then held in place with screws, wires, pins, or metal
plates attached to the outside of the bone.
Bone graft. If some of the bone has been lost through the wound or is crushed, the fracture may
require bone graft to fill the gaps. Bone graft can be taken from a donor (allograft) or from
another bone in your own body (autograft)—most often the hip. In some cases, an artificial material
can be used.
Removal of the fracture fragment. If the broken bone fragment is too small to repair, it is sometimes
removed. When this is done, the triceps tendon, which is attached to the fragment, is reattached to
the remaining portion of the ulna.
Complications of surgery
There are risks associated with all surgery. If your doctor recommends surgery, he or she thinks that
the possible benefits outweigh the risks.
Potential complications include:
Infection. There is a risk of infection with any surgery. Your doctor will take specific
measures to help prevent infection.
Hardware irritation. A small percentage of patients may experience irritation from the metal
implants used to repair the fracture.
Damage to nerves and blood vessels. There is a minor risk of damage to nerves and blood vessels
around the elbow. This is an unusual side effect.
Nonunion. Sometimes, a fracture does not heal. The fracture may pull apart and the screws,
plates, or wires may shift or break. This can occur for a number of reasons, including:
The patient does not follow directions after surgery.
The patient has a health problem, such as diabetes, that slows healing. Smoking or using
other tobacco products also slows healing.
If the fracture was associated with a cut in the skin (open fracture), healing is often
slower.
Infections can also slow or prevent healing.
If the fracture fails to heal, further surgery may be needed.
Recovery
Pain Management
Most fractures hurt moderately for a few days to a couple of weeks. Many patients find that using
ice, elevation (holding their arm up above their heart), and simple, non-prescription medications
for pain relief are all that are needed to relieve pain.
If your pain is severe, your doctor may suggest a prescription-strength medication, such as an
opioid, for a few days.
Be aware that although opioids help relieve pain after surgery, opioid dependency and overdose has
become a critical public health issue. For this reason, opioids are typically prescribed for a short
period of time. It is important to use opioids only as directed by your doctor. As soon as your pain
begins to improve, stop taking opioids.
Rehabilitation
Whether your treatment is surgical or nonsurgical, full recovery from an olecranon fracture requires
a good effort at rehabilitation.
Nonsurgical Treatment
Because nonsurgical treatment can sometimes require long periods of splinting or casting, your elbow
may become very stiff. For this reason, you may need a longer period of physical therapy to regain
motion.
During rehabilitation, your doctor or a physical therapist will provide you with exercises to help:
Improve range of motion
Decrease stiffness
Strengthen the muscles within the elbow
You will not be allowed to lift, push, or pull anything with your injured arm for a few weeks. Your
doctor will talk with you about specific restrictions.
Surgical Treatmen
Depending on the complexity of the fracture and the stability of the repair, your elbow may be
splinted or casted for a short period of time after surgery.
Physical therapy. Patients will usually begin exercises to improve motion in the elbow and
forearm shortly after surgery, sometimes as early as the next day. It is extremely important to
perform the exercises as often as directed. The exercises will only make a difference if they are
done regularly.
Restrictions. You will not be allowed to lift heavy objects with your injured arm for at least
6 weeks. You will also be restricted from pushing and pulling activities, such as opening doors or
pushing up while rising from a chair. You may be allowed to use your arm for bathing, dressing, and
feeding activities. Your doctor will give you specific instructions. He or she will also let you
know when it is safe to drive a car.
Complications of Olecranon Fractures
Even with successful treatment, some patients with olecranon fractures may experience long-term
complications.
Loss of Motion
In some cases, a patient may not be able to regain full motion in the affected elbow. In most of
these cases, the patient cannot fully extend or straighten his or her arm. Fortunately, the loss of
a few degrees of straightening does not usually affect the overall function of the arm. Patients who
have significant loss of motion may require intensive physical therapy, special bracing, or further
surgery. This is uncommon for olecranon fractures.
Posttraumatic Arthritis
Posttraumatic arthritis is a type of arthritis that develops in a joint after an injury. Even when
your bones heal normally, the cartilage lining the joint surfaces can be damaged, leading to pain
and stiffness over time.
Posttraumatic arthritis is a relatively common complication of olecranon fractures. It can occur
shortly after the fracture occurs or can take years to develop. Some patients with posttraumatic
arthritis may need further surgery to relieve their symptoms. However, for many patients, there is
little pain and no need for further treatment.
Outcomes
Most patients can return to their normal activities within about 4 months, although full healing can
take more than a year. Recovering strength in your arm often takes longer than might be expected.
Although x-rays may show that the fracture has healed completely, some patients report that they
still have limitations in movement. These patients will usually continue to improve over time.
Fractures of the coronoid process
Mechanism of injury
The mechanism of injury is as for elbow dislocation and such fractures are associated with elbow
dislocation in about 40% of cases.
Clinical features
Patients present with tenderness over the antecubital fossa and swelling about the elbow.
Check strength of the radial pulse with the elbow at 90°.
Investigations
Lateral X-ray of the elbow should demonstrate a coronoid fracture.
Management
Non-displaced fractures should be immobilised in a long arm posterior splint with the elbow at
90° and the forearm in full supination. After three weeks, start active range of movement
exercises using a sling for comfort.
Displaced fractures or those involving >50% of process need surgical repair.
Fractures of the distal humerus
Mechanism of injury
Supracondylar/transcondylar - most are extension-type injuries from a fall on to an outstretched
arm.
Transcondylar fractures are more common in the elderly.
Supracondylar fractures are more common in children.
Clinical features
The patient usually presents with elbow swelling and pain.
Undertake careful examination for neural or vascular involvement due to risk of damage to the
brachial artery and nerve.
Marked swelling of the forearm or palpable induration of forearm flexors, with pain on passive
extension of the fingers, suggests acute volar compartment syndrome requiring emergency
fasciotomy.
Up to 18% of humeral shaft fractures have an associated radial nerve palsy.
Investigations
AP and lateral X-rays of the elbow.
Management
All but non-displaced or minimally displaced fractures without neural or vascular involvement
should be referred for surgical repair - although a Cochrane review found a lack of consensus on
best surgical management.
Immobilise the elbow in a long arm posterior splint with the elbow at 90° to the forearm in
neutral rotation.
Check distal pulses after the splint has been applied and, if absent, extend the elbow to the
point where pulses return.
Frequent checking of neural and vascular function is essential during the first 7-10 days, and
ice and elevation are important in reducing swelling.
Re-examine within 24-48 hours.
After two weeks, patients should remove the splint and perform gentle exercises, continuing to
use a splint for approximately six weeks, and then starting vigorous exercises.
Intercondylar fractures
These are T- or Y-shaped fractures with varying displacement between the condyles and the humerus.
Mechanism of injury
Commonly caused by a direct or indirect blow to the elbow. The olecranon is forced as a wedge between
the two condyles of the humerus.
Clinical features
The patient usually presents with marked tissue swelling, holding their forearm in pronation.
The injured forearm may appear shortened.
Crepitus of movement may be felt when condyles are pressed together.
Investigations
AP and lateral views should reveal the intercondylar fracture.
Management
Most fractures require surgery because they are displaced[7].
Refer for orthopaedic opinion.
Rarely, non-displaced fractures can be treated similarly to non-displaced supracondylar
fractures, as above.
Condylar fractures
Mechanism of injury
Lateral condyle fractures are more common than medial.
Lateral fractures are usually due to a sudden varus stress on an elbow in extension.
Medial fractures are due either to impact to the olecranon with a flexed elbow or sudden valgus
stress on an elbow in extension.
Clinical features
Patients usually present with swelling, limited range of movement and tenderness over the
injured condyle.
Crepitus with motion is frequently present.
Investigations
AP and lateral X-rays reveal a widened intercondylar distance and there may be displaced
fracture fragments.
Management
Aspiration of joint haemarthrosis relieves discomfort.
Displaced fractures require surgical correction
Undisplaced fractures can be treated with a long arm posterior splint with the elbow at 90°.
Capitellum fracture
Mechanism of injury
These fractures are usually caused by a fall on to the outstretched hand or by direct trauma
Clinical features
These fractures involve the distal humeral articular surface.
Present with anterior elbow pain and effusion.
Investigations
Lateral and AP radiography usually reveals the fracture.
Management
Undisplaced fractures may be splinted but more usually they are displaced and require surgical
fixation.
Elbow dislocation
Elbow dislocation is the second most common major joint dislocation. The 'terrible triad of the
elbow' refers to a combination of elbow dislocation and radial head and coronoid process fracture -
it is notoriously difficult to manage although a systematic review found that whilst
complications
are common, functional outcomes are generally satisfactory.
A simple dislocation does not have any major bone injury.
A complex dislocation can have severe bone and ligament injuries.
Mechanism of injury
Often due to a fall on to an extended elbow.
Those without fracture are termed simple, whereas dislocations with fracture are termed complex.
They are classified according to position of the ulna in relation to the humerus after injury.
Clinical features
Often associated with injury to brachial artery and nerve, so undertake a full examination of
distal pulses, and median and ulnar nerve function.
The patient usually presents with severe pain, with the elbow flexed and swelling and deformity
apparent.
Investigations
AP and lateral X-rays of the elbow to confirm dislocation and exclude fractures.
Management
Prompt reduction is essential. This is usually performed under IV sedation and with adequate
analgesia.
Posterior dislocation:
First try countertraction on the humerus while applying longitudinal traction on the wrist
and forearm.
Continue distal traction as the elbow is flexed.
May need downward pressure on the proximal forearm.
If this fails, place the patient face down with the elbow hanging off the side of the table
and place a small pillow under the humerus just proximal to the elbow joint; hang a 2.5-10
kg weight from the wrist or apply gentle longitudinal traction.
Usually reduces within several minutes but may need forward pressure on the olecranon.
Anterior dislocation:
Basically the reverse of the above, applying posterior and downward pressure to the forearm
whilst applying anterior pressure from behind to the distal humerus.
After reduction, test joint mobility and stability and check neural and vascular function.
Repeat X-ray and immobilise the elbow in a posterior splint with the elbow at 90°.
Ream and Run
Introduction:
The ream and run procedure is a hemiarthroplasty of the shoulder. It is a partial replacement of the
shoulder joint (ball and socket mechanism). During this procedure the humeral head (ball) is
replaced with a metallic ball in an attempt to restore (a) smoothness of the surface (b) sphericity
of the humeral head.
The metallic implant has a stem that is press fitted into the
bone canal – humeral canal. The
prosthetic metallic head is attached to the stem of the implant with a morse taper
mechanism.
Arthritis of the humeral head – ball with loss of sphericity and smoothness of the ball
The procedure was pioneered by Dr Frederick Matsen at the University of Washington (UW) in Seattle
for patients who want to maintain high levels of activity and are too young to have a full
replacement of the shoulder. A full replacement of the shoulder for those individuals may lead to
early failure of the implant on the socket side. During the ream and run procedure the glenoid is
reamed and smoothened. This socket smoothening in conjuction with the replacement of the humeral
head -ball of the shoulder, allows for smooth articulation of the joint. Patients are carefully
selected for this procedure as it does require intense therapy and the recovery time is somewhere
between 6-12 months. The most common problem seen with this type of surgery is stiffness of the
shoulder which may require manipulation or conversion to a total shoulder replacement.
Individuals who want to maintain high levels of activity can contact me to find out if they
are good
candidates for this surgery. Generally, it is not offered to smokers, patients with multiple medical
problems, females as they have a tendency to have less than an ideal outcome. Prior surgery to the
shoulder is also a relative contra-indication for this type of surgery.
During my training at the UW I had the chance to participate in a large number of those
surgeries
and I am grateful for the experience I received there.
Indications:
A ream and run hemiarthroplasty is commonly used in the following clinical scenarios
Arthritis of the shoulder in a young patient, <60-65 years old, with high levels of activity
No prior surgery or injury to the shoulder.
it is not offered to smokers, patients with multiple medical problems, females as they have a
tendency to have less than an ideal outcome.
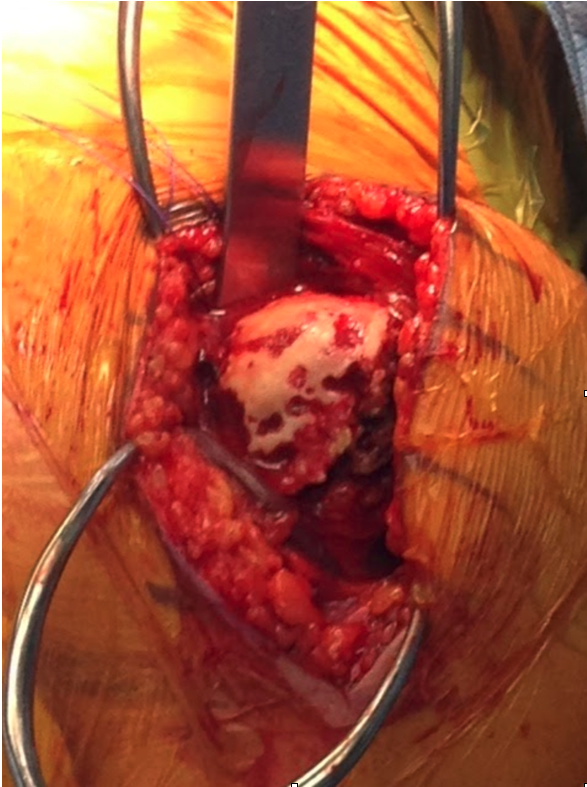
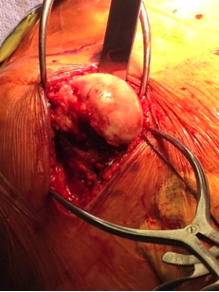
Technique:
An arthroscope (camera) was placed in this shoulder as indicated below. The video shows the
formation of fibrocartilage on the socket side after the ream and run operation. This patient had an
arthroscopy in attempt to obtain culture specimens to evaluate for possible infection. On the top
left corner of the screen you can see the prosthetic humeral head and on bottom the socket with the
fibrocartilage formation.
The following animation shows how the implant is inserted in the humeral canal and press fitted.
Rehabilitation:
The rehabilitation after the ream and run hemiarthroplasty requires immobilization of the shoulder
in a sling for 6 weeks. During that time passive and assistive range of motion is permited. Like the
conventional hemiarthroplasty, this is necessary to allow the muscles of the shoulder to heal as
those are separated and then repaired after implantation of the prosthesis. It is crucial to avoid
forceful internal or external rotation of the shoulder- such as opening or closing doors with the
arm. During those 6 weeks the sling can be removed for therapy and passive range of motion of the
shoulder. After 6 weeks the sling is discontinued and light strengthening is started with
progressive supine bench pressing, as well as scapular muscle and deltoid muscle strengthening.
Patients experience the full benefit of surgery between 6-12 months from surgery.
Results:
The results of ream and run hemiarthroplasty in terms of relief of pain are less predictable but
very close to those of a total shoulder replacement – replacing the ball and socket of the shoulder.
However, the benefit of the ream and run hemiarthroplasty is that it does not require any limitation
in activity. After 6 months patients are allowed to do anything they wish to do. With the total
shoulder replacement heavy activity is not permitted as this level of activity will result in early
failure of the implant. The relief in pain from a ream and run hemiarthroplasty can be full, however
most of the time is partial. The main reasons for a revision of a ream and run hemiarthroplasty is
stiffness, erosion of the socket – glenoid of the shoulder- from the metallic ball, infection, or
hardware complications such as loosening. Stiffness can be managed sometimes with gentle
manipulation under conscious sedation. The frequency of those complications is somewhere between
4-10%.
Modal Heading
Modal body..
Hand Surgery
The hand conditions that may affect the quality of life of a patient are plenty. These are too
numerous to describe them in a single document. For more information on certain conditions of the
hand that may require surgery please follow the handcare patient education portal developed by the
American Society for Surgery of the Hand.
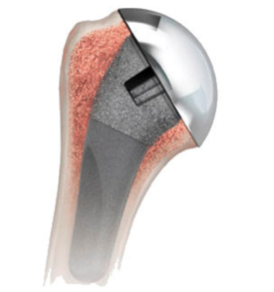
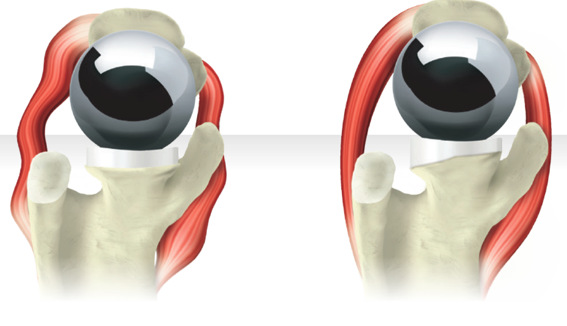
Total Shoulder Replacement
Introduction:
The total shoulder replacement is a common procedure performed for glenohumeral joint arthritis. It
is a full replacement of the shoulder joint (ball and socket mechanism). During this procedure the
humeral head (ball) is replaced with a metallic ball in an attempt to restore (a) smoothness of the
surface (b) sphericity of the humeral head. The socket is resurfaced and a polyethylene implant is
implanted that allows articulation with the metallic ball. This articulation is much more efficient
in decreasing friction within the glenohumeral joint as compared to the hemiarthoplasty – partial
replacement, or ream and run procedure.
The metallic implant has a stem that is press fitted into the bone canal – humeral canal. The
prosthetic metallic head is attached to the stem of the implant with a morse taper mechanism.
Illustration above shows the ball and socket prosthetic articulation. On the right the
socket have a wedged implant.
Arthritis of the humeral head – ball with loss of sphericity and smoothness of the ball
Patients who want to maintain high levels of activity and are too young to have a full replacement
of the shoulder are not good candidates for this procedure. A full replacement of the shoulder for
those individuals may lead to early failure of the implant on the socket side. That happens because
studies have shown that 5-10 years after surgery there is micromotion and loosening of the implant
placed on the socket, there is also wear – linear and volumetric. Interestingly, not all shoulders
that have loosening of the glenoid component – socket implant have pain
Patients are carefully selected for this procedure as it does require compliance with therapy and
the recovery time is somewhere between 6-12 months. The most common problem seen with this type of
surgery is progressive loosening of the glenoid component- socket implant.This may or may not
require revision surgery in the distant future. The survivorship of this surgery is about 80-90% at
10 years after surgery.
Individuals who want to perform basic level of daily activity and have arthritis of the shoulder can
contact me to find out if they are good candidates for this surgery. Generally, it is not offered to
smokers, patients with multiple medical problems that prevent us from providing general anesthesia,
chronic narcotic opioid use, loss of bone stock on the socket side of the shoulder, loss of the
rotator cuff tendons, active or previous serious infection of the shoulder.
Generally good candidates for this surgery are patients who are of low demand and older than 65
years old who do not work a heavy duty job and do not perform heavy duty activity in general.
Indications:
A total shoulder replacement is commonly used in the following clinical scenarios
Arthritis of the shoulder in a patient, >60-65 years old, with low levels of daily activity
No prior infection to the shoulder.
Patients who have less than ideal outcomes are: Smokers, patients with multiple medical
problems, multiple prior surgeries to the shoulder, active infection to the shoulder, chronic
opioid use, loss of cartilage to the shoulder due prior trauma or surgery to the shoulder.
Technique:
This is an animation of computer planning of the anatomic total shoulder replacement. This was
generated using my software called OrthoMesh3D which it is used for detailed 3D surgical planning.
It is part of the online course used by students from 21 countries on how to plan such an
operation.(Udemy Website)
The following animation shows how the implant is inserted in the humeral canal and press
fitted.
Rehabilitation:
The rehabilitation after the total shoulder replacement requires immobilization of the shoulder in a
sling for 6 weeks. During that time passive and assistive range of motion is permitted. Like the
conventional hemiarthroplasty, this is necessary to allow the muscles of the shoulder to heal as
those are separated and then repaired after implantation of the prosthesis. It is crucial to avoid
forceful internal or external rotation of the shoulder- such as opening or closing doors with the
arm. During those 6 weeks the sling can be removed for therapy and passive range of motion of the
shoulder. After 6 weeks the sling is discontinued and light strengthening is started with
progressive supine bench pressing, as well as scapular muscle and deltoid muscle strengthening.
Patients experience the full benefit of surgery between 6-12 months from surgery.
Results:
The results of total shoulder replacment in terms of relief of pain are very good with complete or
near complete relief of pain. After 6 months patients are allowed to do anything they wish to do as
long as it is not heavy-duty activity that places a lot of stress on the operated shoulder. With the
total shoulder replacement heavy activity is not permitted as this level of activity will result in
early failure of the implant. The relief in pain from a total shoulder replacement can be full,
however most of the time is near full. The main reasons for a revision of a total shoulder
replacement loosening of the socket side implant, usually 5-10% at 10 years after surgery –Potential
complications are: infection, or hardware complications such as loosening, fracture or stiffness.
Stiffness can be managed sometimes with gentle manipulation under conscious sedation. The frequency
of those complications is somewhere between 4-10%. Based on my collected data from the surgeries I
performed between 2016-2019 my complication rate is 5%.
CARPAL TUNNEL SYNDROME
Carpal tunnel syndrome is a common condition that causes pain, numbness, and tingling in the hand and
arm. The condition occurs when one of the major nerves to the hand — the median nerve — is squeezed
or compressed as it travels through the wrist.
In most patients, carpal tunnel syndrome gets worse over time, so early diagnosis and treatment are
important. Early on, symptoms can often be relieved with simple measures like wearing a wrist splint
or avoiding certain activities.
If pressure on the median nerve continues, however, it can lead to nerve damage and worsening
symptoms. To prevent permanent damage, surgery to take pressure off the median nerve may be
recommended for some patients.
Most cases of carpal tunnel syndrome are caused by a combination of factors. Studies show that women
and older people are more likely to develop the condition.
Other risk factors for carpal tunnel syndrome include:
Heredity. This is likely an important factor. The carpal tunnel may be smaller in some people or
there may be anatomic differences that change the amount of space for the nerve—and these traits
can run in families.
Repetitive hand use. Repeating the same hand and wrist motions or activities over a prolonged
period of time may aggravate the tendons in the wrist, causing swelling that puts pressure on
the nerve.
Hand and wrist position. Doing activities that involve extreme flexion or
extension of the hand and wrist for a prolonged period of time can increase pressure on the
nerve.
Pregnancy. Hormonal changes during pregnancy can cause swelling.
Health conditions. Diabetes, rheumatoid arthritis, and thyroid gland imbalance are conditions
that are associated with carpal tunnel syndrome.
Numbness, tingling, burning, and pain—primarily in the thumb and index, middle, and ring
fingers.
Occasional shock-like sensations that radiate to the thumb and index, middle, and ring fingers.
Pain or tingling that may travel up the forearm toward the shoulder
Weakness and clumsiness in the hand—this may make it difficult to perform fine movements such as
buttoning your clothes.
Dropping things—due to weakness, numbness, or a loss of proprioception (awareness of where your
hand is in space).
In most cases, the symptoms of carpal tunnel syndrome begin gradually—without a specific injury. Many
patients find that their symptoms come and go at first. However, as the condition worsens, symptoms
may occur more frequently or may persist for longer periods of time.
Night-time symptoms are very common. Because many people sleep with their wrists bent, symptoms may
awaken you from sleep. During the day, symptoms often occur when holding something for a prolonged
period of time with the wrist bent forward or backward, such as when using a phone, driving, or
reading a book.
Many patients find that moving or shaking their hands helps relieve their symptoms.
If this condition is left untreated for a long period of time, loss of muscle strength and bulk of
the thenar – base of the thumb can happen, and this is an irreversible condition. See picture
below
During your evaluation, your doctor will talk to you about your general health and medical
history and will ask about your symptoms.
He or she will carefully examine your hand and wrist and perform a number of physical tests. During
these tests, your doctor will:
Press down or tap along the median nerve at inside of your wrist to see if it causes any
numbness or tingling in your fingers (Tinel sign).
Bend and hold your wrists in a flexed position to test for numbness or tingling in your hands.
Test sensitivity in your fingertips and hands by lightly touching them with a special instrument
when your eyes are closed.
Check for weakness in the muscles around the base of your thumb
Look for atrophy in the muscles around the base of your thumb. In severe cases, these muscles
may become visibly smaller.
Electrophysiological tests. These tests will help your doctor measure how well your median
nerve is working and help determine whether there is too much pressure on the nerve. The tests will
also help your doctor determine whether you have another nerve condition, such as neuropathy, or
other sites of nerve compression that might be contributing to your symptoms.
Electrophysiological tests may include:
Nerve conduction studies. These tests measure the signals travelling in the nerves of your hand
and arm and can detect when a nerve is not conducting its signal effectively. Nerve conduction
studies can help your doctor determine how severe your problem is and help to guide treatment.
Electromyogram (EMG). An EMG measures the electrical activity in muscles. EMG results can show
whether you have any nerve or muscle damage.
Ultrasound. An ultrasound uses high-frequency sound waves to help create pictures of bone and
tissue. Your doctor may recommend an ultrasound of your wrist to evaluate the median nerve for
signs of compression.
X-rays. X-rays provide images of dense structures, such as bone. If you have limited wrist
motion or wrist pain, your doctor may order x-rays to exclude other causes for your symptoms,
such as arthritis, ligament injury, or a fracture.
Magnetic resonance imaging (MRI) scans. These studies provide better images of the body's soft
tissues. Your doctor may order an MRI to help determine other causes for your symptoms or to
look for abnormal tissues that could be impacting the median nerve. An MRI can also help your
doctor determine if there are problems with the nerve itself—such as scarring from an injury or
tumor.
Nonsurgical Treatment
If diagnosed and treated early, the symptoms of carpal tunnel syndrome can often be relieved without
surgery. If your diagnosis is uncertain or if your symptoms are mild, your doctor will recommend
nonsurgical treatment first.
Wearing a splint or brace reduces pressure on the median nerve by keeping your wrist straight.
Nonsurgical treatments may include:
Bracing or splinting. Wearing a brace or splint at night will keep you from bending your wrist
while you sleep. Keeping your wrist in a straight or neutral position reduces pressure on the
nerve in the carpal tunnel. It may also help to wear a splint during the day when doing
activities that aggravate your symptoms.
Nonsteroidal anti-inflammatory drugs (NSAIDs). Medications such as ibuprofen and naproxen can
help relieve pain and inflammation.
Activity changes. Symptoms often occur when your hand and wrist are in the same position for too
long—particularly when your wrist is flexed or extended.
If your job or recreational activities aggravate your symptoms, changing or modifying these
activities can help slow or stop progression of the disease. In some cases, this may involve making
changes to your work site or work station.
A steroid injection into the carpal tunnel may relieve symptoms for a period of time.
Nerve gliding exercises. Some patients may benefit from exercises that help the median nerve move
more freely within the confines of the carpal tunnel. Specific exercises may be recommended by your
doctor or therapist.
Steroid injections. Corticosteroid, or cortisone, is a powerful anti-inflammatory agent that can be
injected into the carpal tunnel. Although these injections often relieve painful symptoms or help to
calm a flare up of symptoms, their effect is sometimes only temporary. A cortisone injection may
also be used by your doctor to help diagnose your carpal tunnel syndrome.
Surgical Treatment
If nonsurgical treatment does not relieve your symptoms after a period of time, your doctor may
recommend surgery.
The decision whether to have surgery is based on the severity of your symptoms—how much pain and
numbness you are having in your hand. In long-standing cases with constant numbness and wasting of
your thumb muscles, surgery may be recommended to prevent irreversible damage.
Surgical Procedure
The surgical procedure performed for carpal tunnel syndrome is called a "carpal tunnel release."
There are two different surgical techniques for doing this, but the goal of both is to relieve
pressure on your median nerve by cutting the ligament that forms the roof of the tunnel. This
increases the size of the tunnel and decreases pressure on the median nerve.
In most cases, carpal tunnel surgery is done on an outpatient basis. The surgery can be done under
general anesthesia, which puts you to sleep, or under local anesthesia, which numbs just your hand
and arm. In some cases, you will also be given a light sedative through an intravenous (IV) line
inserted into a vein in your arm.
Open carpal tunnel release. In open surgery, your doctor makes a small incision in the palm of your
hand and views the inside of your hand and wrist through this incision. During the procedure, your
doctor will divide the transverse carpal ligament (the roof of the carpal tunnel). This increases
the size of the tunnel and decreases pressure on the median nerve.
After surgery, the ligament may gradually grow back together—but there will be more space in the
carpal tunnel and pressure on the median nerve will be relieved.
Recovery
Immediately following surgery, you will be encouraged to elevate your hand above your heart and move
your fingers to reduce swelling and prevent stiffness.
You should expect some pain, swelling, and stiffness after your procedure. Minor soreness in your
palm may last for several weeks to several months.
Grip and pinch strength usually return by about 2 to 3 months after surgery. If the condition of your
median nerve was poor before surgery, however, grip and pinch strength may not improve for about 6
to 12 months.
You may have to wear a splint or wrist brace for several weeks. You will, however, be allowed to use
your hand for light activities, taking care to avoid significant discomfort. Driving, self-care
activities, and light lifting and gripping may be permitted soon after surgery.
Complications
Although complications are possible with any surgery, your doctor will take steps to minimize the
risks. The most common complications of carpal tunnel release surgery include:
Bleeding
Infection
Nerve aggravation or injury
Outcomes
For most patients, surgery will improve the symptoms of carpal tunnel syndrome. Recovery, however,
may be gradual and complete recovery may take up to a year.
If you have significant pain and weakness for more than 2 months, your doctor may refer you to a hand
therapist who can help you maximize your recovery.
If you have another condition that causes pain or stiffness in your hand or wrist, such as arthritis
or tendonitis, it may slow your overall recovery. In long-standing cases of carpal tunnel syndrome
with severe loss of feeling and/or muscle wasting around the base of the thumb, recovery will also
be slower. For these patients, a complete recovery may not be possible.
Occasionally, carpal tunnel syndrome can recur, although this is rare. If this happens, you may need
additional treatment or surgery.
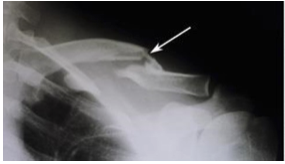
Clavicle Fractures
Introduction:
Collarbone or clavicle fractures are common injuries. A broken clavicle is the result of direct blow
to the bone. These injuries are seen in sports, falls from heights, motorcycle or automobile
accidents or altercations.
Diagnosis:
The diagnosis is established using x-rays
Treatment
Nonsurgical Treatment
If the broken ends of the bones have not significantly shifted out of place, you may not need
surgery. Most broken collarbones can heal without surgery.
Nonsurgical treatment may include:
Arm support. A simple arm sling is usually used for comfort immediately after the break and to
keep your arm and shoulder in position while the injury heals.
Medication. Pain medication, including acetaminophen, can help relieve pain as the fracture
heals.
Physical therapy. Although there will be some pain, it is important to maintain arm motion to
prevent stiffness. Often, patients will begin doing exercises for elbow motion immediately after
the injury.
After a clavicle fracture, it is common to lose some shoulder and arm strength. Once the bone begins
to heal, your pain will decrease and your doctor may start gentle shoulder exercises. These
exercises will help prevent stiffness and weakness. More strenuous exercises will be started
gradually once the fracture is completely healed.
Follow-up care. You will need to see your doctor regularly until your fracture heals. During
these visits, he or will take x-rays to make sure the bone is healing in a good position. After the
bone has healed, you will be able to gradually return to your normal activities.
Complications. In some cases, a clavicle fracture can move out of place before it heals. It is
important to follow up with your doctor as scheduled to make sure the bone stays in position.
If the fracture fragments do move out of place and the bones heal in that position, it is called a
"malunion." Treatment for this is determined by how far out of place the bones are and how much this
affects your arm movement.
A large bump over the fracture site may develop as the fracture heals. This usually gets smaller over
time, but a small bump may remain permanently.
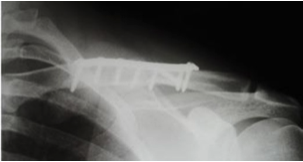
Surgical Treatment
If the broken ends of the bones have significantly shifted out of place, your doctor may recommend
surgery.
Surgery typically involves putting the broken pieces of bone back into position and preventing them
from moving out of place until they are healed. This can improve shoulder strength when you have
recovered.
Open reduction and internal fixation. This is the procedure most often used to treat clavicle
fractures. During the procedure, the bone fragments are first repositioned (reduced) into their
normal alignment. The pieces of bone are then held in place with special metal hardware.
Common methods of internal fixation include:
Plates and screws. After being repositioned into their normal alignment, the bone fragments are
held in place with special screws and metal plates attached to the outer surface of the bone.
After surgery, you may notice a small patch of numb skin below the incision. This numbness will
become less noticeable with time. Because the clavicle lies directly under the skin, you may be able
to feel the plate through your skin.
Plates and screws are not routinely removed after the bone has healed, unless they are causing
discomfort. Problems with the hardware are not common, but some patients find that seatbelts and
backpacks can irritate the collarbone area. If this happens, the hardware can be removed after the
fracture has healed.
(Left) X-ray shows a displaced clavicle fracture (arrow). (Right) The pieces of bone have been
realigned and held in place with plates and screws.
Pins or screws. Pins or screws can also be used to hold the fracture in good position after the
bone ends have been put back in place. The incisions for pin or screw placement are usually
smaller than those used for plates.
Pins or screws often irritate the skin where they have been inserted and are usually removed
once the fracture has healed.
Pain management. After surgery, you will feel some pain.This is a natural part of the healing
process. Many patients find that using ice and simple, non-prescription medications for pain relief
are all that is needed to relieve pain.
If your pain is severe, your doctor may suggest a prescription-strength medication, such as an
opioid, for a few days.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be
addictive. Opioid dependency and overdose has become a critical public health issue. For this
reason, opioids are typically prescribed for a short period of time. It is important to use opioids
only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids.
Rehabilitation. Specific exercises will help restore movement and strengthen your shoulder. Your
doctor may provide you with a home therapy plan or suggest that you work with a physical
therapist.
Therapy programs typically start with gentle motion exercises. Your doctor will gradually add
strengthening exercises to your program as your fracture heals.
Although it is a slow process, following your physical therapy plan is an important factor in
returning to all the activities you enjoy.
Complications. There are risks associated with any type of surgery. These include:
Infection
Bleeding
Problems with wound healing
Pain
Blood clots
Damage to blood vessels or nerves
Reaction to anesthesia
Difficulty with bone healing
Lung injury
Hardware irritation
Patients who smoke or use tobacco products, have diabetes, or are elderly are at a higher risk for
complications both during and after surgery. They are also more likely to have problems with wound
and bone healing.
Before your surgery, your doctor will discuss each of the risks with you and will take specific
measures to avoid complications.
Outcome
Whether your treatment involves surgery or not, it can take several months for your collarbone to
heal. Healing may take longer in diabetics or in people who smoke or use tobacco products.
Most people return to their regular activities within 3 months of their injury. Your doctor will tell
you when your injury is stable enough to do so. Returning to regular activities or lifting with your
arm before your doctor advises may cause the fracture fragments to move or the hardware to break.
This may require you to start your treatment from the beginning.
Once your fracture has completely healed, you can safely return to sports activities.
Rotator Cuff Tear
Introduction:
The rotator cuff problems are very common in the general population. They are usually seen in
patients who older than 40-50 years of age. It is estimated that 3.5 billion dollars are spent each
year in the US to treat the rotator cuff tears. There are 250000 rotator cuff repairs performed each
year in the US. This has a very significant impact to the society, if we consider that the cost of
fighting diabetes mellitus in the US is 45 billion dollars per year.
The rotator cuff is a group of muscles that control the motion of the shoulder. The role of the
rotator cuff in the motion of the shoulder has been studied extensively. The main function of the
rotator cuff is initiation of the shoulder motion.
The video below illustrates the anatomy of the rotator cuff:
There are different types of tear. Partial thickness tear almost like a pair of blue jeans that has
wear and tear but not complete tear and full thickness tear that involves the entire tendon-
essentially the tendon is detached from the bone.
Those tears are further subdivided to acute and chronic tears. An acute tear is a tear that is less
than 4-6 weeks old and it is the result of a specific traumatic event. Those tears need surgery
urgently, - not emergently.
Chronic tears of the rotator cuff are either traumatic which are more than 4-6 weeks old or
degenerative in nature which means wear and tear over the course of years.
Statistical analysis and epidemiologic studies have shown 50-60% chance of degenerative tears after
the age of 65 and 30% chance of both shoulders involved.
While it is clear that a traumatic tear needs surgery, we currently do not know whether all
degenerative tears need surgery. Some degenerative tears develop so slowly over the course of years
that the patient does not have pain or has minimal pain and no loss of motion or strength to the
shoulder. Those tears usually do not require surgery.
Rotator cuff tears-Frequently asked questions
What is the function of the rotator cuff?
The ball and socket mechanism of your shoulder joint is covered by several tendons. These
tendons are 4 and combined together they form a "cuff" over the upper part of the ball
(humerus). These muscles originate from the scapula (shoulder blade) and insert on the ball.
Their main function is to rotate the ball of the shoulder. They also provide stability to the
shoulder.
How did I get a rotator cuff tear?
There are two types of rotator cuff tears. Those that are related to a trauma that caused the
tear (heavy lifting etc) and those that happen due to wear and tear of the tendons over time.
After the age of 40 the wear and tear process in your shoulder tendon begins and by age 65
approximately 50% of population will have a partial or complete rotator cuff tear.
How is it possible for so many people to have a rotator cuff tear and not have problems?
There are patients who have a rotator cuff degenerative tear and have no symptoms. A clear
explanation does not exist, however it is possible that these patients compensate for the lost
tendon with the other tendons. If the degenerative process is slow enough the other tendons may
compensate for the loss.
If my MRI shows a rotator cuff tear and have no symptoms what should I do?
This tear is called an asymptomatic tear. A tear that is compensated. In that case your doctor
will re-evaluate you every few months to make sure that the tear does not became symptomatic. As
long you have no symptoms NO SURGERY IS NECESSARY.
If I have a painful rotator cuff and keep using it, will this cause further damage?
A rotator cuff tear can extend or get larger over time. This can occur with repetitive use or a
re-injury. It is common for patients with known rotator cuff disease to have acute pain and
weakness following a minor injury. This likely represents extension of an existing tear.
If you know you have a rotator cuff tear, then worsening pain and decreasing strength may mean
the tear is getting larger.
When should I see a doctor for a rotator cuff tear?
If your shoulder had no pain and you start having pain or if you had a tear that caused no
symptoms and you start having pain then you should see an orthopaedic surgeon. It is important
to monitor the symptoms and the size of the tear from the onset of symptoms because if the tear
gets larger it is more difficult to treat and has tendency to re-tear.
What can I do if I do not need surgery for the tear? How can I make it better?
Treatment can be done without surgery and improve symptoms if strengthening of the other tendon
muscles is achieved with physical therapy or home therapy. The tendon will not heal but the
symptoms may improved. In additon, anti-inflammatories or cortizone injections may be given
however these have only temporary relief.
At what point does a rotator cuff tear require surgery to fix it?
There several situations that need surgery. A well functioning shoulder that losses strength and
motion after an injury to the joint is an indication to do surgery. The traumatic tears need to
be repaired within the first 2-4 weeks after the injury. If a degenerative tear is not
responding to therapy and conservative treatment or changes in size and becomes bigger overtime
then surgery will be required.
Patients who older than the age of 65, are diabetes, chronic use of opioids, have a history of
smoking or arthritis to the shoulder are not good candidates for surgery. They have lower
satisfaction rates and higher re-tear rates over time. Active patients who use the arm for
overhead work or sports are more in need for repair.
What is it done during surgery and how is it done?
Your doctor will examine your shoulder, discuss with you your lifestyle activities and other
medical problems. He will also evaluate the tendons with an MRI and tell you what type of
treatment you need. The surgical treatment options are outlined below and can be done with an
arthroscopy (telescope) or with open surgery - mini or traditional open. There is no data to
show that one method is better over the other:
(1) trimming or smoothing procedure called a débridement.
(2) A full-thickness tear within the substance of the tendon can be repaired side to side. If
the tendon is torn from its insertion on the humerus, it is repaired directly to bone.
(3) Use of tissue to augment the tendon repair. The results are not encouraging in terms of
healing in the long term/run
(4) Partial repair. If the tendon is not long enough to be repaired back to bone then a partial
repair is done.
How important is rehabilitation in the treatment of a rotator cuff tear?
Following your doctors protocol of surgical repair is critical especially protecting your arm
for the first 6 to 12 weeks after the surgery. Studies show that early motion of your arm versus
late motion of your arm has no effect on the result of your surgery. Exercise of your arm when
it is safe for the repair will strengthen your other tendons and protect your repair.
How often will I be attending physical therapy? For how long?
In most cases you will attend physical therapy 1-3 times a week for 8-12 weeks post-op.
Sometimes the program may last for 6 months after your surgery.
Are hot or cold packs better for my shoulder after surgery?
Hot packs sometimes feel "good" to the shoulder. However, studies show that the swelling of the
shoulder reduces with the use of cold packs.
When can I begin to drive?
Approximately 4-6 weeks from time of surgery. The criteria for driving are as follows:
Once you are no longer taking narcotic pain medications during the day.
Ability to safely control steering wheel with minimal use of involved shoulder and no
discomfort doing so.
Automatic transmission only during the first 4-6 weeks.
When can I go back to work after surgery?
Depending on whether or not light duty is available, you could return as soon as 1-2 weeks. If
your occupation requires raising of arms overhead, reaching or lifting, then approximately 8-12
weeks.
Will I need to wear a sling for any extended period of time?
For the first 6 weeks it is critical to wear your sling that will protect you from a possible
injury to the repair in case of a fall or accident. Your doctor may modify this time frame based
on the size of the tear and your progress of healing.
When can I begin to raise/lift the arm on my own after the surgery?
For 6 weeks no motion of your arm is allowed by activating your own muscles (doing it on your
own). The physical therapist will raise the arm for you and you will not apply any force. If you
have no physical therapy prescribed you need to assist with your other arm to lift the arm for
the first 6 weeks.
When will I be able to return to sports, conditioning and recreation after the surgery?
Sports that require high contact and impact are not allowed until 6 months after surgery.
Overhead activities that require throwing a ball are not allowed until 4 months after surgery.
Technique:
An arthroscope (camera) was placed is placed in the shoulder, anchors are used the repair of the
tendon to the bone. The incisions are about the size of the tip of a finger the surgery takes
1-2 hours. Most of the time if the health status of the patients allows the surgery is done in
the outpatient setting.
Rehabilitation:
The rehabilitation after the rotator cuff repair requires immobilization of the shoulder in a
sling for 6 weeks. During that time passive and assistive range of motion is permitted. It is
necessary to allow the tendons of the shoulder to heal prior to heavy activity. It is crucial to
avoid forceful rotation of the shoulder- such as lifting with the arm for 6-12 weeks. During the
first 6 weeks the sling can be removed for therapy and passive range of motion of the shoulder.
After 6 weeks the sling is discontinued and light strengthening is started. Patients experience
the full benefit of surgery between 6-12 months from surgery.
Results:
The results of rotator cuff repair in terms of relief of pain can be 80-90% relief of pain.
After 6 months patients are allowed to do anything they wish to do. The main reasons for a
revision of a rotator cuff repair, is recurrent tear. Infection is below 2-3%, stiffness is
possible if the therapy is not done after surgery. Stiffness can be managed sometimes with
gentle manipulation under conscious sedation after 6 months from surgery.
Labrum Tear
Introduction:
Since orthopedic surgeons began using a tiny TV camera called an arthroscope to diagnose and treat
shoulder problems, they have discovered several conditions that no one knew existed. One of these
conditions is an injury to a small structure in the shoulder called the labrum. A labral tear can
cause pain and a catching sensation in the shoulder. Labral tears can be very difficult to diagnose.
This document will help you understand:
where and what the labrum is
what tests your doctor will run to diagnose the problem
what you can do to relieve your pain
Anatomy
What is the labrum?
The shoulder is made up of three bones: the scapula (shoulder blade), the humerus (upper arm
bone),
and the clavicle (collarbone).
A part of the scapula, called the glenoid, makes up the socket of the shoulder. The glenoid is very
shallow and flat. The labrum is a rim of soft tissue that makes the socket more like a cup. The
labrum turns the flat surface of the glenoid into a deeper socket that molds to fit the head of the
humerus.
The rotator cuff connects the humerus to the scapula. The rotator cuff is formed by
the tendons of four muscles: the supraspinatus, infraspinatus, teres minor, and subscapularis.
Tendons attach muscles to bones. Muscles move the bones by pulling on the tendons. The rotator cuff
helps raise and rotate the arm. As the arm is raised, the rotator cuff also keeps the humerus
tightly in the glenoid of the scapula.
The soft labral tissue can be caught between the glenoid and the humerus. When this happens, the
labrum may start to tear. If the tear gets worse, it may become a flap of tissue that can move in
and out of the joint, getting caught between the head of the humerus and the glenoid. The flap can
cause pain and catching when you move
your shoulder. Several tendons and ligaments attach to the labrum that help maintain the stability
of the shoulder. So when the labrum tears, the shoulder often becomes much less stable.
Causes
What causes labral tears?
Labral tears are often caused by a direct injury to the shoulder, such as falling on an outstretched
hand. The labrum can also become torn from the wear and tear of activity, a condition
called overuse. An injured labrum can lead to shoulder instability. The extra motion of the humerus
within the socket causes additional damage to the labrum. An extremely unstable shoulder may slip or
dislocate. This can also cause the labrum to tear.
The biceps tendon attaches to the front part of the labrum. The biceps is the large muscle
on the front of your upper arm. Sports can cause injuries to the labrum when the biceps tendon pulls
sharply against the front of the labrum. Baseball pitchers are prone to labral tears because the
action of throwing causes the biceps tendon to pull strongly against the top part of the labrum.
Weightlifters can have similar problems when pressing weights overhead. Golfers may tear their
labrum if their club strikes the ground during the golf swing.
Symptoms
What does a labral tear feel like?
The main symptom caused by a labral tear is a sharp pop or catching sensation in the shoulder during
certain shoulder movements. This may be followed by a vague aching for several hours. At other
times, the tear may not cause any pain. Shoulder instability from a damaged labrum may cause the
shoulder to feel loose, as though it slips with certain movements.
Diagnosis
What tests will my doctor run?
Your doctor may suspect a labral tear based on your medical history. You will be asked questions
about your pain and past injuries to your shoulder that may suggest labral damage.
In the physical examination, there are several shoulder movements that can bring on the symptoms. You
may feel a catching sensation as your arm is raised, and there may be pain when the arm is held
overhead. If your arm is held in front of your body, with the palm of the hand facing downward, you
may feel pain when your doctor tries to push down on your arm.
Labral tears are difficult to see, even in a magnetic resonance imaging (MRI) scan. An MRI scan is a
special imaging test that uses magnetic waves to show the tissues of the shoulder in slices. The MRI
scan shows soft tissues such as tendons and ligaments as well as bones.
Labral tears may be seen using computed tomography (CT) scan and a special dye. A CT scan is an older
test that uses computer-enhanced X-rays to show slices of the shoulder. The soft tissues do not show
up in a CT scan, but the special dye does. The dye shows the outline of the labrum. If there is a
tear, the dye may leak into it and show up on the CT scan.
However, MRI and CT scans are not very accurate in detecting labral tears. Confirming the diagnosis
of a labral tear can be extremely difficult. A surgeon may need to look into your shoulder using
an arthroscope. The arthroscope is a small TV camera that is inserted into the shoulder joint
through a very small incision. The surgeon can then see pictures of the joint on a TV screen. This
allows the surgeon to look directly at the labrum to see if it is torn.
Treatment
What treatment options are available?
Nonsurgical Treatment
Your doctor's first goal will be to control your pain and inflammation. Initial treatment for pain
control is usually rest and anti-inflammatory medication, such as aspirin or ibuprofen. Your doctor
may suggest a cortisone injection if you have trouble getting your pain under control. Cortisone is
a strong anti-inflammatory medication. It can provide good relief, although its effects are
temporary.
Your doctor will probably have a physical or occupational therapist direct your rehabilitation
program. Your first therapy treatments will try to ease pain and inflammation by using such
treatments as heat or ice. Hands-on treatment and various types of exercises are used to improve the
range of motion in your shoulder and the nearby joints and muscles.
Later, you will do strengthening exercises to improve the strength and control of the rotator cuff
and shoulder blade muscles. Your therapist will help you retrain these muscles to keep the ball of
the humerus in the glenoid. This will improve the stability of your shoulder and help it move
smoothly during all your activities.
You may need therapy treatments for four to six weeks. Most patients are able to get back to their
activities with full use of their arm within this amount of time.
Surgery
If your symptoms don't go away, you may need surgery. Surgical treatment for this condition is still
evolving. Surgeons have not known about the problem long enough to adequately evaluate the results
of different treatments.
Labral Debridement
The arthroscope can be used to treat many labral tears. If the tear is small and is mostly getting
caught as you move the shoulder, simply removing the frayed edges and any loose parts of the labrum
may get rid of your symptoms. This is called labral debridement.
Labral Repair
If the tear is larger, the shoulder may also be unstable. If this is the case, the labral tear may
need to be repaired, rather than simply removed. Several new techniques allow surgeons to place
small staples or anchors into the labrum through an arthroscope. The staples/anchors attach the
labrum to the bone of the glenoid.
Open Procedure
If the tear is too large to repair through the arthroscope, the surgeon will need to make
an incision in the front of the shoulder. The main drawback of making the larger incision is that it
will probably take you longer to recover from surgery.
Rehabilitation
What should I expect after treatment?
Nonsurgical Rehabilitation
Even nonsurgical treatment requires a rehabilitation program. Some evidence suggests that shoulder
instability may eventually make labral tears worse. The goal of therapy will be to strengthen the
rotator cuff muscles to make the shoulder more stable. At first you will do exercises with the
therapist. Eventually you will be put on a home program of exercise to keep the muscles strong and
flexible. This should help you avoid future problems.
After Surgery
Rehabilitation after surgery is more complex. You may need to wear a sling to support and protect the
shoulder for a few days after surgery. A physical or occupational therapist will probably direct
your recovery program. Depending on the surgical procedure, you will probably need to attend therapy
sessions for one to two months, and you should expect full recovery to take up to three months.
Getting the shoulder moving as soon as possible is important. However, this must be balanced with the
need to protect the healing tissues. The first few therapy treatments will focus on controlling the
pain and swelling from surgery. Ice and electrical stimulation treatments may help. Your therapist
may also use massage and other types of hands-on treatments to ease muscle spasm and pain.
Therapy proceeds quickly after a simple arthroscopic surgery to clean up the frayed edges or loose
parts of the labrum. Sessions start with range-of-motion exercises and gradually work into active
stretching and strengthening. Overhand athletes start their sports gradually within four to six
weeks. They can usually return to competition within three months.
After surgery to repair the labrum, therapists usually begin with passive exercises. In passive
exercises, the shoulder joint is moved, but your muscles stay relaxed. Your therapist gently moves
your joint and gradually stretches your arm. You may also be taught how to do passive exercises at
home.
Active therapy starts about six weeks after repair surgery. Active range-of-motion exercises help you
regain shoulder movement using your own muscle power. Light isometric strengthening exercises are
started about this time. These exercises work the muscles without straining the healing joint.
By about the tenth week, you will start more active strengthening. Exercises will focus on improving
strength and control of the rotator cuff muscles. They help tighten the ball of the humerus in the
glenoid socket and can improve the stability of the shoulder. A stronger and more stable shoulder
helps keep the ball of the humerus centered in the socket during all your activities.
Some of the exercises you will do are designed get your shoulder working in ways that are similar to
your work tasks and sport activities. Your therapist will help you find ways to do your tasks that
don't put too much stress on your shoulder. Before your therapy sessions end, your therapist will
teach you a number of ways to avoid future problems.
Modal Heading
Modal body..
Hemiarthroplasty
Introduction:
Malunions are conditions in which the fractured bone heals in non acceptable angulation that may
compromise the function of the limb. These are conditions in which the patient seeks medical
attention due to loss of motion, function, strength or development of pain.
Diagnosis:
The diagnosis is established with plain xrays, however it is not uncommon for a surgeon to order a CT
scan and perform a 3D reconstruction of the bone in attempt to better understand the deformity. This
process is crucial in complex conditions especially when surgery is planned.
I am the developer of an add on module for the animation software called Blender. This software
allows for surgical planning in 3D and for better understanding of the condition. Based on the 3D
bone models that are generated in the computer cutting guides can be produced that allow accurate
corrections of the deformity, decrease operating room time and bleeding.
Below are some videos of the software used for this purpose
Total Shoulder Replacement
Introduction:
The reverse total shoulder replacement is a relatively new procedure approved by the FDA to be used
in the US in 2004. Prior to that date and in the 1980s Paul Grammont in France designed and
established the reverse total shoulder replacement that we use today. Several attempts were done
before, starting in the 1970s but most of these early designs had catastrophic failures.
What is a reverse total shoulder replacement?
As illustrated in the above picture (A) the anatomic total shoulder replacement
consists of a metallic ball and a socket – glenoid component- that mimics the shoulder joint
(ball and socket mechanism). The reverse total shoulder prosthesis provides stability to the
shoulder when the rotator cuff is absent and the joint is arthritic. As shown in picture (B) it
has a ball where the socket normally is and the socket where normally the ball is. So, it is
reversed. This new design changes the center of rotation of the shoulder. In comparison to the
(A) configuration it moves the center of rotation of the joint closer to the shoulder blade or
socket. This change allows the deltoid muscle to work as a “rotator” muscle. In this case, when
this procedure is done in patients who have (a) loss of the rotator cuff tendons (b) arthritis
of the shoulder joint (c) limited range of shoulder joint, the deltoid muscle works as a rotator
cuff and allows the patient to elevate the arm higher, sometimes all the way up. Prior to 2004
we did not have a solution for this complex shoulder condition called -rotator cuff arthropathy
– which is the combined clinical conditions (a), (b) and (c).
The picture below shows the changes in the biomechanics of the shoulder seen after reverse total
shoulder replacement.
During this procedure the humeral head (ball) is replaced with a socket that has a polyethylene
component in it and the glenoid receives a metallic ball called the glenosphere in an attempt to (a)
restore smoothness of the joint surface to address the arthritis (b) provide stability of the
shoulder and (c) to move the center of rotation closer to the scapula and make the deltoid muscle
effectively rotate the arm.
The metallic implant has a stem that is press fitted into the bone canal – humeral canal. The
prosthetic socket is attached to the stem of the implant with a morse taper mechanism.
Arthritis of the humeral head – ball with loss of rotator cuff muscles
Indications:
A reverse total shoulder replacement is commonly used in the following clinical scenarios
Arthritis of the shoulder in an elderly patient, >70 years old, with low levels of activity
Patients who are older than 70 years old and have loss of the rotator cuff muscles that are not
amendable to repair due to retraction poor tendon quality and quantity.
Patient with the above problem in conjuction with arthritis of the shoulder – this condition is
called rotator cuff arthropathy.
It is not offered to patients with have frequent fall, patients with multiple medical problems,
fracture of the shoulder blader, or injury to the deltoid muscle or its nerves.
Technique:
An incision is made in the front of the shoulder, the muscles are separated and the bone is cut and
replaced with metallic as indicated in the animation below.
Rehabilitation:
After the reverse total shoulder replacement the shoulder is immobilized in a sling for 6 weeks.
During that time passive and assistive range of motion is permitted to the elbow and wrist. Like the
conventional anatomic arthroplasty, this is necessary to allow the muscles of the shoulder to heal
as those are separated after implantation of the prosthesis. It is crucial to avoid forceful
internal or external rotation of the shoulder- such as opening or closing doors with the arm, or
pushing off a chair with the operated shoulder. During those 6 weeks the sling can be removed for
therapy and passive range of motion of the elbow and wrist. After 6 weeks the sling is discontinued
and light strengthening is started with progressive supine bench pressing, as well as scapular
muscle and deltoid muscle strengthening. Patients experience the full benefit of surgery between
6-12 months from surgery.
Results:
The results of reverse total shoulder replacement in terms of relief of pain are excellent and very
close to those of a total shoulder replacement – replacing the ball and socket of the shoulder.
However, the benefit of the reverse total shoulder replacement is that it does not require any
extensive therapy. The limitation is that weight lifting of more than 20 pounds is not permitted for
life. This is a salvage surgery to provide elevation of the arm and pain relief, it is not designed
for high levels of activity. Heavy activity is not permitted as this level of activity will result
in early failure of the implant. The relief in pain from a reverse total shoulder replacement can be
full, and sometimes the elevation of the shoulder is full as well. However, most of the time is
partial. The main reason for a revision of a reverse total shoulder replacement is instability which
used to be 30%, however the last 4-5 years with the newer implants it is only 6% when the surgery is
done for arthritis. Other complications are stiffness, infection, or hardware complications such as
loosening or fracture of the bone. The frequency of all complications is somewhere between 4-10%.
Shoulder Elbow Arthroscopy
Introduction:
Arthroscopy of the shoulder is a minimally invasive procedure that allows diagnosis and treatment of
diseases of the shoulder or elbow joint. It is performed with a “telescope” – known as arthroscope.
The arthroscope is a surgical instrument that has a small camera attached at the tip. By making a
small incision about the size or half the size of the tip of the index finger we can insert the
arthroscope in the joint and see inside the joint. Please see video below about the definition and
technique of shoulder arthroscopy.
Benefits of shoulder arthroscopy:
When arthroscopy was introduced in surgery it was seen with criticism. Many orthopaedic surgeons
believed that it is a “toy”. Now, arthroscopy is one of the major advances in the field of
orthopaedic surgery as it is proven to be safe, it allows for faster recovery of the shoulder and
more accurate diagnosis of shoulder conditions. Many procedures that were done in the past through
large open incisions now they are done through small incisions. Examples of those are rotator cuff
repair, repair of torn labrum, removal of loose bodies, decompression of nerves, etc.. Infection in
shoulder arthroscopy is very rare, less than 1%
Below you can watch a presentation about fixation a fracture of the socket – glenoid of the shoulder
though a small camera- arthroscope. This from the technique that I developed and published in the
Journal of Arthroscopy.
link
Benefits of elbow arthroscopy:
Using elbow arthroscopy we can treat a variety of joint diseases such as loose bodies, tennis elbow,
smoothening of the elbow joint, release of scar tissue to improve range of motion and even resection
of the bone. It is minimal invasive and allows the patient to move the elbow immediately with fast
recovery which is 6-8 weeks depending the reason that the surgery is performed. There is very
minimal risk of infection , around or less than 1%
What are the risks of arthroscopy of the elbow or shoulder:
The main risks of shoulder and elbow arthroscopy is nerve injury. It is very uncommon in shoulder
arthroscopy less than 1%. During my 10-year practice I have never had one patient that I injured a
nerve around the shoulder during arthroscopic shoulder surgery. In elbow arthroscopy it is about 4%
for transient numbness to the arm that resolves over a few weeks and about 1% risk of major nerve
damage. In a clinical study of 253 elbow arthroscopies in which I participated as a co-author there
were only a few cases with permanent elbow nerve damage. Over a 10-year period, 253 elbow
arthroscopies were performed at Wake Forest University Hospital. Minor and major nerve-related
complications were recorded. There were 12 reported peripheral nerve injuries, 10 minor (4.4%) and 2
major complications (0.9%).
link
What about bone spurs of the shoulder or "shoulder impingement"
For updated information on this condition follow
this link.
How long does it take to heal from shoulder or elbow arthroscopy
The surgical wounds usually heal in 14 days. Rotator cuff repair that is done through the
arthroscope has a healing rehab time of 6 months. By 6 weeks patients remove the sling that they
were and they can drive. The same timeframe applies for labrum tears of the shoulder.
Elbow arthroscopy has healing times somewhere between 6-12 weeks. Usually the sling is removed within
one week and the wounds on the skin heal in 14 days.
Other minor procedures of the elbow or shoulder such as removal of loose bodies cleaning of the
shoulder or removal of bone spurs have shorter recovery times, usually 6 weeks.
How long does it take to perform elbow or shoulder arthroscopy
It depends on the experience of the shoulder or elbow surgeon and the complexity of the problem being
treated. When I started practicing orthopaedic surgery in my early years an arthroscopic rotator
cuff repair would take me 2 ½ hours now the fastest I have performed such a repair is 35 minutes.
Elbow arthroscopy takes somewhere between 30-60 minutes to be performed.
What kind of anesthesia do patients have for shoulder or elbow arthroscopy
Depending on the preference of the patient surgeon and anesthesiologist elbow arthroscopy can be
performed using local regional nerve block and/or general anesthesia. For the shoulder arthroscopy
general anesthesia is required and the presence of a nerve block depends on the preference of the
patient and anesthesiologist.
Proximal Humerus Fracture
Introduction:
Most fractures of the proximal humerus can be treated without surgery if the bone fragments are not
shifted out of position (displaced). If the fragments are shifted out of position, surgery is
usually required. Surgery usually involves fixation of the fracture fragments with plates, screws,
or pins or it involves shoulder replacement
How does the surgeon decide what treatment is best for me?
The treatment methods are:
immobilization in sling
fixation with plates and screws or nails
shoulder replacement
The most significant determining factors about the best option are
age of the patient
concurrent injuries
activity level and profession of the patient
health status
balance problems
controlled vs uncontrolled diabetes
presence of a nerve injury around the shoulder
prior history of shoulder arthritis
configuration of the fracture, displacement, number of fragments etc